The Complete Guide to Equine Joint Health: Anatomy, Pathology, Management, and Therapy
The horse is an evolutionary masterpiece of biomechanical engineering. Designed for rapid travel across vast distances, a horse’s skeletal structure relies on a complex system of levers and fulcrums to absorb immense ground reaction forces while maintaining forward momentum. At the very center of this athletic system sits the equine joint.
Whether you are managing a Grand Prix dressage horse, a competitive cutting horse, a racehorse running at top speeds, or a beloved trail partner enjoying senior retirement, preserving joint health is your single most important responsibility. Joint dysfunction—specifically osteoarthritis—remains the leading cause of lameness, early retirement, and compromised quality of life in horses worldwide.
This comprehensive pillar guide breaks down the biological framework of the equine joint, details the pathology of degenerative joint disease, explores diagnostic methods, and reviews modern management, nutritional, and pharmaceutical options available to safeguard your horse’s long-term soundness.
1. Anatomy and Physiology of the Equine Joint
To effectively protect a horse’s joints, we must first understand how they are built and how they function. The horse has three main categories of joints: fibrous (immovable, like the sutures of the skull), cartilaginous (semi-movable, like the pelvic symphysis), and synovial (freely movable, like the hock, stifle, and fetlock).
For performance and soundness, our primary focus is on the synovial joint.
The Five Key Structural Components
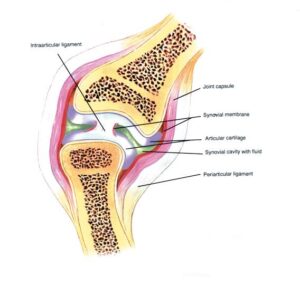
Every healthy synovial joint relies on a delicate balance of five fundamental components, as shown in the diagram above:
-
Articular Cartilage: A highly specialized, smooth, blue-white connective tissue covering the ends of the bones within the joint. It is unique because it is completely devoid of blood vessels, lymphatics, and nerves (avascular and aneural). It relies entirely on cellular diffusion to receive nutrients. Cartilage consists of cells called chondrocytes embedded within an extracellular matrix of Type II collagen fibers and hydrophilic (water-attracting) proteoglycans.
-
Subchondral Bone: The dense bone layer situated immediately underneath the articular cartilage. It acts as a supportive cushion, flexing subtly under load to dissipate shock forces that pass through the cartilage surface.
-
The Synovial Membrane (Synovium): The delicate, vascularized inner lining of the joint capsule. It acts as a selective biological filter, allowing nutrients from the bloodstream to enter the joint while producing the vital molecules needed for lubrication.
-
Synovial Fluid: A viscous, clear-to-pale-yellow fluid that fills the joint cavity. It serves two vital tasks: lubricating the moving surfaces to minimize friction and acting as a vehicle for nutrient and waste transport for the avascular chondrocytes.
-
The Fibrous Joint Capsule and Ligaments: The tough, protective outer sleeve that encloses the joint. It provides mechanical stability, prevents hyper-extension, and contains nerve endings that convey spatial awareness (proprioception) to the horse’s brain.
The Role of Glycosaminoglycans (GAGs) and Hyaluronic Acid
The fluid dynamics of an equine joint depend on specialized molecules. The cartilage matrix is packed with chondroitin sulfate and keratan sulfate, which are specialized sugars known as glycosaminoglycans (GAGs). These GAGs attach to a central core to form huge aggregates called aggrecans.
Because these molecules possess a strong negative electrical charge, they repel each other while forcefully attracting and trapping water molecules. Think of it like a dense molecular sponge: when the horse steps down, water is squeezed out of the cartilage matrix to form a protective liquid cushion. When the hoof leaves the ground, the electrical charges pull the water straight back in.
Simultaneously, the synovium secretes Hyaluronic Acid (HA) and a protective protein called lubricin directly into the synovial fluid. This gives the fluid its thick, slippery quality, ensuring that the friction coefficient within a healthy joint is lower than that of ice sliding on ice.
2. High-Risk Zones: Key Joints of the Equine Athlete
While a horse has dozens of moving joints, specific areas bear the brunt of athletic stress. Understanding which joints are most vulnerable in individual disciplines allows caretakers to monitor them closely.
The Hock (Tarsus)
The hock is one of the hardest-working joints in the horse’s body, functioning as the primary generator of forward thrust and hind-leg leverage.
It is a complex joint comprised of four distinct articulations:
-
-
Tibiotarsal Joint: The large, highly mobile top joint that accounts for nearly all the hock’s flexing capability.
-
Proximal Intertarsal Joint: A low-motion joint situated just below the tibiotarsal joint.
-
Distal Intertarsal Joint: A low-motion joint in the lower hock.
-
Tarsometatarsal Joint: The lowest-motion joint, interfacing directly with the cannon and splint bones.
-
As seen in the anatomical structure above, the lower three joints are low-motion joints. Because they bear massive compressive forces without significant bending, they are highly prone to bone-on-bone compression. This frequently leads to a form of osteoarthritis colloquially known as bone spavin. Show jumpers, dressage horses, and reining horses place extreme load on these low-motion joints during collection, making them high-risk zones.
The Stifle (Femorotibial and Femoropatellar)
The equivalent of the human knee, the stifle is the largest and most complex joint in the horse. It consists of the femoropatellar joint (where the kneecap slides) and the femorotibial joint (divided into medial and lateral compartments).
The stifle relies heavily on fibrocartilage pads called menisci and an intricate web of collateral and cruciate ligaments for stability. Stifle issues are common in eventing, steeplechase, and performance horses that must navigate deep footing or execute rapid changes of direction. Common problems include upward fixation of the patella (“locked stifles”) and meniscal tears.
The Fetlock (Metacarpophalangeal/Metatarsophalangeal Joint)
The fetlock is a high-motion ginglymus (hinge) joint subjected to profound hyperextension during high-speed gaits. At a full gallop or over a large fence, the fetlock drop is so extreme that the back of the joint can touch the ground surface. This results in intense compression of the articular cartilage on the front of the joint and severe tension on the suspensory apparatus at the back. It is a primary hotspot for racehorses, barrel racers, and polo ponies, often leading to synovitis, osselets, and osteochondral fragments (bone chips).
The Coffin Joint (Distal Interphalangeal Joint)
Encased entirely within the rigid hoof capsule, the coffin joint experiences significant rotational and shear stresses, particularly on uneven ground or if the hoof is poorly balanced. Coffin joint inflammation (capsulitis or osteoarthritis) is a major contributor to low-grade, bilateral front-limb lameness in performance horses across all major disciplines.
3. The Pathology of Osteoarthritis and Degenerative Joint Disease
Joint degradation is rarely a sudden event; rather, it is a progressive, insidious cycle that can occur silently for months or even years before causing noticeable lameness. While veterinarians use terms like synovitis, capsulitis, osteoarthritis (OA), and Degenerative Joint Disease (DJD), these represent different stages along a single destructive pathway.
The Cascade of Destruction
The osteoarthritic cascade can be initiated by a single acute injury (such as a severe twist in the pasture) or repetitive, sub-clinical micro-trauma from routine training.
[Repetitive Trauma / Acute Injury]
│
▼
[Synovitis & Capsulitis] ──► (Releases Cytokines: IL-1, TNF-α)
│
▼
[Activation of Matrix Metalloproteinases (MMPs)]
│
▼
[Cartilage Degradation] ──► (Fibrillation & Erosion)
│
▼
[Subchondral Bone Sclerosis] ──► (Osteophytes & Bone Remodeling)
-
Synovitis and Capsulitis: The initial phase involves inflammation of the joint lining (synovium) and outer capsule. The inflamed synovium floods the joint cavity with inflammatory cytokines, particularly Interleukin-1 (IL-1) and Tumor Necrosis Factor-Alpha (TNF-$\alpha$).
-
Enzymatic Attack: These cytokines signal the chondrocytes to stop building cartilage and start producing destructive enzymes: Matrix Metalloproteinases (MMPs) and Aggrecanases. These enzymes act like microscopic scissors, cutting through the protective collagen and proteoglycan framework.
-
Fluid Thinning: Concurrently, the inflamed synovium stops producing high-molecular-weight hyaluronic acid. The joint fluid loses its characteristic viscosity, turning thin, watery, and acidic. The joint loses its primary lubrication mechanism, resulting in direct friction during movement.
-
Cartilage Fibrillation and Erosion: Deprived of protective fluid lubrication and under enzymatic assault, the articular cartilage begins to fray (fibrillate). Vertical cracks develop, and eventually, whole pieces of cartilage wear away, exposing raw, underlying bone.
-
Bone Remodeling (Osteophytes): Because cartilage has no nerve supply, early stages are relatively painless. However, as cartilage erodes, the sensitive subchondral bone undergoes intense shock. The bone responds by thickening and hardening (sclerosis). In an attempt to stabilize the unstable joint, the body spurs abnormal bone growth at the joint margins—these are known as osteophytes or bone spurs. At this stage, chronic pain and permanent mechanical restriction set in.
4. Recognizing the Signs: How to Spot Joint Issues Early
Waiting for a horse to show a overt, head-bobbing lameness means missing the golden window for early medical intervention. As caretakers, we must develop a sharp eye for subtle behavioral and physical clues that point to early joint distress.
Physical Manifestations
-
Joint Effusion (“Windpuffs” or “Bog Spavin”): When a joint is inflamed, it attempts to cool itself by over-producing synovial fluid. This results in soft, fluid-filled swellings around the joint capsule. While common, an unexpected increase in effusion is a clear warning sign of active synovitis.
-
Localized Heat and Pain on Palpation: Regularly feeling your horse’s limbs after work allows you to spot subtle heat over specific joints. Applying gentle manual pressure or flexing a joint manually can reveal a hidden pain response, such as a flinch or leg withdrawal.
-
Reduced Range of Motion: Over time, chronic joint inflammation leads to a thickening of the joint capsule. If you note that a horse can no longer comfortably flex its hock to your chest or extend its front limb forward during grooming, joint capsule fibrosis may be developing.
Behavioral and Performance Clues
Horses are masters at hiding pain. Often, joint discomfort presents as a change in behavior or training resistance:
-
Difficulty in Lead Changes: Sudden trouble executing clean flying lead changes often indicates hock or stifle pain, as the horse struggles to push off and engage its hindquarters.
-
“Cold-Backed” Behavior or Resistance to Saddling: Hocks and stifles connect directly to the mechanics of the pelvic limb and spine. A horse experiencing hind-limb joint pain will hollow its back, resist rounding, or display irritation when the girth is tightened.
-
Reluctance to Travel Downhill: Forelimb joint issues (especially coffin and fetlock pain) become dramatically worse when traveling down inclines, as gravity shifts the horse’s weight forward onto the front legs.
-
Loss of Impulsion and Shorter Stride Length: An arthritic horse may not limp noticeably on one leg if both sides hurt equally. Instead, their entire stride becomes short, choppy, and uncoordinated—owners often describe the feeling as “riding on stilts.“
5. Diagnostic Techniques in Modern Equine Veterinary Medicine
If you suspect joint issues, a professional veterinary evaluation is paramount. Modern equine medicine utilizes a systematic combination of clinical exams and advanced imaging technology to map out joint pathology.
The Complete Lameness Evaluation
A comprehensive assessment begins with a thorough physical examination and visual evaluation:
-
Palpation and Conformation Analysis: The vet checks for asymmetry, swelling, heat, and structural faults that create uneven joint loading.
-
Visual Evaluation: The horse is observed walking and trotting in straight lines and on hard and soft lunging circles. Lunging on a hard surface emphasizes lower-limb pain (coffin/fetlock), while soft footing often accentuates upper-limb issues (stifle/shoulder).
-
Flexion Tests: The veterinarian holds a specific joint in an extreme flexed position for 30 to 60 seconds, then immediately trots the horse off. By temporarily stressing the joint capsule, a flexion test amplifies hidden discomfort, helping locate the source of lameness.
Diagnostic Nerve and Joint Blocks
To confirm that a specific joint is causing pain, veterinarians perform local anesthesia. Using sterile techniques, a local anesthetic (such as Mepivacaine) is injected directly into the joint capsule (intra-articular block). If the horse trots out completely sound 15 minutes after the block, the veterinarian has confirmed the exact site of the pain.
Imaging Modalities: From X-Rays to MRI
Once the pain is localized, imaging allows the vet to evaluate the internal structures:
| Imaging Tool | Best Used For | Limitations |
| Digital Radiography (X-Rays) | Visualizing bone structure, osteophytes, joint space narrowing, and subchondral bone sclerosis. | Cannot see cartilage, early synovitis, or soft-tissue tears. |
| Ultrasound | Evaluating joint capsules, collateral ligaments, menisci (stifles), and the surface contours of bone. | Cannot penetrate through dense bone to see deep inside the joint. |
| Nuclear Scintigraphy (Bone Scan) | Detecting areas of high bone turnover or hidden remodeling (hotspots) across the entire skeleton. | Provides excellent localization but lacks fine structural detail. |
| Magnetic Resonance Imaging (MRI) | The gold standard for mapping out cross-sectional views of both bone and soft tissue simultaneously. | Expensive; typically requires general anesthesia or standing sedation at a clinic. |
| Computed Tomography (CT) | Generating pristine 3D reconstructions of complex bony architecture (excellent for hocks and fetlocks). | Limited availability; requires specialized large-animal equipment. |
6. Systematic Treatment: The Equine Joint Therapeutic Pyramid
Managing joint health successfully requires a multi-layered approach. Think of it as a therapeutic pyramid: you start with a baseline of foundational care and add targeted medical treatments as the severity of the disease demands.
/ \
/ \ Stage 4: Surgical Intervention (Arthrodesis / Debridement)
/ \
/ \ Stage 3: Targeted Intra-Articular Biologics (IRAP, PRP, Stem Cells)
/ \
/ \ Stage 2: Systemic DMOADs & Medications (HA, Pentosan, NSAIDs)
/ \
/ \ Stage 1: Foundational Management (Farriery, Diet, Oral Supplements)
/_________________\
Stage 1: Foundational Management
The absolute bedrock of joint health consists of daily management choices that reduce mechanical wear and tear.
Precision Farriery
The foot dictates the strain placed on every joint up the leg. An unbalanced hoof creates asymmetric loading across the joint surface. For example, a low-heel, long-toe conformation delays the hoof’s breakover phase, causing severe, prolonged hyperextension of the coffin and fetlock joints.
Regular trimming and shoeing every 4 to 6 weeks—focused on maintaining perfect lateral balance and an optimal phalangeal axis—is mandatory.
Weight Optimization
Every extra pound a horse carries translates to exponentially increased concussive forces traveling through their joints. Maintaining a horse at a healthy Body Condition Score (BCS) of 5 on the Henneke scale drastically lessens the structural strain on compromised hind limbs.
Turnout and Movement Strategy
Stall confinement is a primary contributor to joint stiffness. Continuous, low-impact motion during pasture turnout keeps the joint capsule supple and ensures a constant cycling of synovial fluid. Performance horses benefit from longer, dedicated walk warm-ups (minimum 15-20 minutes) before any high-intensity training begins.
7. Oral Joint Supplements: Navigating the Ingredients
The equine oral joint supplement industry is immense, making it challenging for owners to separate marketing hype from scientific reality. When scanning ingredient labels, look for therapeutic substances with documented clinical data.
1. Glucosamine (HCI and Sulfate)
Glucosamine is an amino sugar that serves as a fundamental building block for glycosaminoglycans (GAGs) within the cartilage matrix. Research indicates that glucosamine can assist chondrocytes in synthesizing new matrix tissue and may provide a mild anti-inflammatory effect inside the joint capsule.
2. Chondroitin Sulfate
Chondroitin is the primary GAG found within articular cartilage, responsible for giving the tissue its water-attracting, shock-absorbing capabilities. It works synergistically with glucosamine, helping block the catabolic enzymes that break down existing cartilage structures.
3. Methylsulfonylmethane (MSM)
MSM is an organic sulfur compound renowned for its potent antioxidant and anti-inflammatory properties. While it does not rebuild cartilage directly, it helps scavenge free radicals within inflamed joint capsules, reducing pain and post-exercise stiffness.
4. Hyaluronic Acid (HA)
Oral high-molecular-weight hyaluronic acid can be absorbed systemically in horses. It targets the fluid dynamics of the joint, helping restore the viscosity of the synovial fluid and acting as a mild systemic anti-inflammatory.
5. Avocado Soy Unsaponifiables (ASU)
ASU is a natural vegetable extract derive from avocado and soybean oils. It is a highly regarded oral ingredient for its ability to inhibit inflammatory cytokines (like IL-1) and protect chondrocytes from enzymatic degradation, frequently outperforming glucosamine and chondroitin alone in clinical trials.
The Supplement Caveat: Unlike prescription pharmaceuticals, oral supplements are not strictly regulated. Look for reputable brands that utilize third-party purity testing (such as NASC certification) to ensure that what is listed on the label is actually inside the bucket.
8. Pharmaceutical Interventions: Systemic and Targeted Treatments
When foundational management and oral supplements are no longer enough to keep a horse comfortable, targeted medical therapies become necessary. These are divided into systemic treatments (given into the muscle or vein) and local treatments (injected directly into the joint).
Systemic Medications: Injectable DMOADs
Systemic injectables provide excellent, whole-body joint support, protecting multiple joints simultaneously without the localized risks associated with joint punctures.
-
Pentosan Polysulfate Sodium (e.g., Arthropen Vet 250): A highly effective Disease-Modifying Osteoarthritis Drug (DMOAD). Pentosan actively blocks cartilage-destroying enzymes, improves blood flow to the subchondral bone, and triggers the body to produce its own high-quality hyaluronic acid. It is administered via a convenient weekly intramuscular (IM) loading series for 4 weeks, followed by monthly maintenance.
-
Polysulfated Glycosaminoglycans (e.g., Adequan): A classic, heavily researched IM injectable DMOAD derived from bovine tracheal cartilage. It acts as a structural matrix builder, binding directly to damaged cartilage surfaces to stimulate repair while shutting down enzymatic degradation. The standard protocol requires an intensive cycle of 1 injection every 4 days for a total of 7 treatments.
-
Intravenous Hyaluronic Acid (e.g., Legend): This pure, high-molecular-weight HA is administered directly into the jugular vein (IV). It acts as a rapid, powerful anti-inflammatory across all joint linings, breaking down the acute cycle of synovitis and restoring immediate fluid lubrication right before competitive events.
Localized Treatments: Intra-Articular Corticosteroids
For targeted relief of a single, severely arthritic joint, veterinarians frequently use intra-articular injections. Historically, corticosteroids have been the primary choice for this procedure:
-
Triamcinolone Acetonide: A highly potent, fast-acting anti-inflammatory corticosteroid. It is frequently paired with hyaluronic acid for low-motion joints, providing rapid pain relief and breaking down intense local inflammation.
-
Methylprednisolone Acetate: A long-acting corticosteroid often selected for low-motion joints (like the lower hocks) where long-term management is preferred.
A Note on Corticosteroids: While corticosteroids are unrivaled at stopping inflammation, excessive or high-dose use in high-motion joints can sometimes depress chondrocyte metabolism, leading to long-term cartilage drying. For this reason, modern veterinary medicine often favors regenerative options for high-motion areas.
9. Regenerative Medicine: The Frontier of Joint Therapy
Over the past two decades, equine sports medicine has shifted heavily toward biologics—using the horse’s own cellular machinery to heal its joints, minimizing the reliance on traditional synthetic drugs.
1. IRAP (Interleukin-1 Receptor Antagonist Protein)
IRAP is an innovative autologous (derived from the patient’s own body) serum therapy. The veterinarian draws a sample of the horse’s blood into a syringe packed with specialized medical glass beads. These beads stimulate the white blood cells to produce massive quantities of a protective protein called Interleukin-1 Receptor Antagonist Protein.
This protein is harvested, spun down in a centrifuge, frozen into sterile doses, and injected back into the horse’s inflamed joint. IRAP acts as a physical shield, binding directly to the joint’s cellular docking sites to completely block the destructive IL-1 cytokines from attacking the cartilage matrix.
2. PRP (Platelet-Rich Plasma)
PRP is created by spinning a blood sample to isolate a highly concentrated layer of platelets. Platelets are biological storehouses packed with growth factors, including Transforming Growth Factor-Beta (TGF-$\beta$) and Vascular Endothelial Growth Factor (VEGF). When injected into a joint, PRP dampens chronic inflammation, stimulates cellular replication, and accelerates structural tissue regeneration. It is highly valued for managing complex joints with concurrent soft-tissue injuries, such as a stifle with a meniscal tear.
3. Stem Cell Therapy (MSC)
Mesenchymal Stem Cells (MSCs) are harvest from the horse’s own bone marrow or adipose (fat) tissue, or sourced from sterile umbilical cord tissue. These undifferentiated cells are multiplied in a specialized laboratory before being injected directly into a severely damaged joint capsule.
Once inside, stem cells act as a brilliant “biological foreman.” They monitor the micro-environment, release potent anti-inflammatory signals, and coordinate localized cellular repair across heavily compromised cartilage and bone surfaces.
4. Polyacrylamide Gels (e.g., Arthramid Vet)
A highly sophisticated addition to modern equine joint therapy is the use of non-degradable polyacrylamide hydrogels. Unlike medications that treat the fluid or cartilage biochemically, this gel acts mechanically.
Once injected into the joint capsule, the gel migrates through the synovial lining, integrating directly into the fibrous tissue of the joint capsule. This strengthens the outer sleeve, reduces joint capsule transfers under load, and provides long-lasting, mechanical pain relief that can persist for over 12 to 24 months without altering the chemical composition of the joint fluid.
10. Advanced Cases: Surgical Interventions
When a joint reaches end-stage osteoarthritis and all medical therapies fail to provide comfort, surgical interventions can be considered to extend the horse’s life or pasture soundness.
Arthroscopic Debridement
Using small camera ports and specialized tools, an equine orthopedic surgeon can enter a joint capsule to clean up structural debris. They can remove floating osteochondral fragments (bone chips), trim torn meniscal fibers, and smooth down severely frayed cartilage surfaces. This eliminates mechanical irritation and calms the surrounding synovium.
Joint Fusion (Arthrodesis)
For severe, debilitating arthritis in low-motion joints (such as the lower hock joints or the pastern joint), surgical arthrodesis is a highly effective option. The surgeon strips away any remaining cartilage and stabilizes the bones using plates and screws, forcing the bones to grow together into a single, solid block.
Because these joints have very little movement naturally, fusing them eliminates the painful bone-on-bone friction completely without significantly altering the horse’s gaits. Once fully fused, many of these horses can return to comfortable pasture lives or even active performance careers.
11. Creating a Lifecycle Joint Health Plan
Joint care is not a reactive protocol reserve for senior horses; it is a lifecycle strategy that must evolve as your horse grows, matures, and ages.
The Young, Growing Horse (Weanling to 3 Years)
-
Focus: Perfect nutrition and controlled exercise.
-
Strategy: Avoid rapid growth spurts cause by over-feeding high-energy grain concentrates, which can trigger Developmental Orthopedic Diseases (DOD) like Osteochondrosis Dissecans (OCD). Ensure regular farriery to correct angular limb deformities early while the growth plates remain open. Provide maximum pasture turnout to build dense subchondral bone and strong digital tendons.
The Mature Performance Horse (4 to 15 Years)
-
Focus: Proactive protection and monitoring.
-
Strategy: Implement a consistent, structured conditioning program to build supporting muscle mass around key joints. Avoid working on deep, unyielding footing or rock-hard surfaces. Introduce systemic injectable DMOADs (like Pentosan or PSGAGs) prophylactically during peak competitive seasons to manage sub-clinical synovitis before lameness develops. Perform bi-annual veterinary wellness checks to catch subtle changes in range of motion.
The Senior Companion (16+ Years)
-
Focus: Maintaining comfort, mobility, and dignity.
-
Strategy: Never allow an arthritic senior horse to stand immobilize in a stall for long periods. Provide 24/7 turnout with shelter and buddies to keep joints moving naturally. Transition from high-level sports medicine to gentle daily maintenance, using long-term oral supplements (like ASU or MSM) paired with veterinary-prescribed NSAIDs or regular systemic DMOAD injections during cold winter seasons to manage chronic stiffness.
Summary: The Price of Soundness is Eternal Vigilance
Preserving equine joint health requires a dedicated combination of biological understanding, consistent daily management, and timely veterinary medicine. By focusing on correct hoof balance, maintaining a lean body weight, and utilizing a targeted combination of oral supplements, systemic DMOADs, and advanced biologics, you can effectively slow down the osteoarthritic cascade.
Your horse’s joints are the foundation of its athletic ability and physical well-being. Investing in proactive care today ensures a happier, sounder, and more comfortable partner for the track, the arena, or the open trail for years to come.
Top rated
-
 Buy HYGETROPIN 100iu
$130.00
Buy HYGETROPIN 100iu
$130.00
-
 Buy Ascorbate 100mg
$60.00
Buy Ascorbate 100mg
$60.00
-
 Biosal injection
$40.00
Biosal injection
$40.00
-
 Boldenone For Horses
$45.00
Boldenone For Horses
$45.00
-
 tussionex cough syrup
$230.00
tussionex cough syrup
$230.00





